Technical Paper
Fallible pitfalls for novice obstetrician on application of Naegele forceps
1 Department of Obstetrics and Gynecology, Juntendo University Faculty of Medicine, Tokyo, Japan
Address correspondence to:
Jun Takeda
Jun Takeda, Juntendo University Faculty of Medicine, 2-1-1 Hongo, Bunkyo-ku,
Pin- 1138421, Japan
Message to Corresponding Author
Article ID: 100001VAM08JT2018
doi: 10.5348/100001VAM08JT2018TP
Access full text article on other devices

Access PDF of article on other devices

How to cite this article
Takeda J, Ando H, Makino S, Itakura A, Takeda S. Fallible pitfalls for novice obstetrician on application of Naegele forceps. Video J Clin Res 2018;1:100001VAM08JT2018.Abstract
Introduction: Simulation training is one of the choice to acquire a new technique. In our facility, we hold a simulation training program to acquire forceps delivery skill. However, even with the simulation training, the first experience may cause anxiety, and unforeseen event may occur. In this video, we demonstrate a forceps delivery by a novice obstetrician who finished the program, and highlight some important points.
Case Report: The video shows a case of forceps delivery by a novice obstetrician. The forceps delivery was accomplished without any complications. However, there were some points to be improved: insertion of the forceps with the hands reversed, holding the blade instead of the handle, overly shallow placement of the blade, failing to insert the blade with assistance of the right thumb and forcibly inserting the blade with the left hand, overly shallow placement of the blade, adaptation angle is not vertical, failure to hold the end of the handle, and trial of traction force insufficient to confirm fetal head descent.
Conclusion: This video is of use to both instructors and trainees. However, in addition to the video learning, we think that both repetitive simulation training and on-the-job training are important. Novice obstetricians tend to experience similar pitfalls. Thus, it is important for instructors to recognize the pitfalls of trainees. According to the video case, the novice obstetrician did not yet acquire the proper forceps delivery skill. Neither video alone nor simulation training is sufficient for instruction for novice obstetricians in forceps delivery.
Keywords: Education, Naegele forceps, Pitfall, technique, Video
Introduction
Lack of training opportunity impedes acquisition of forceps delivery skills. In our university teaching hospital, we hold a simulation training program every year as well as on the assignment of new obstetricians. Our simulation training program consists of three parts: a lecture, a demonstration, and simulation training experience. The lecture is about pelvic examination for precise assessment of fetal head descent based on trapezoidal fetal station [1], and is supplemented by forceps delivery videos [2], [3]. Then, forceps delivery is demonstrated by instructors, using a pelvic model and fetal doll. Finally, trainees attempt a simulated forceps delivery.
In our facility, residents are required to complete this simulation training program before attempting forceps delivery in actual patients. Furthermore, the first forceps delivery is limited to lower than fetal station +4, and should be supervised by an instructor or an experienced obstetrician. However, the first experience may cause anxiety, and unforeseen event may occur [4]. In this video, we demonstrate a forceps delivery by a novice obstetrician, and highlight some important points.
Case Report
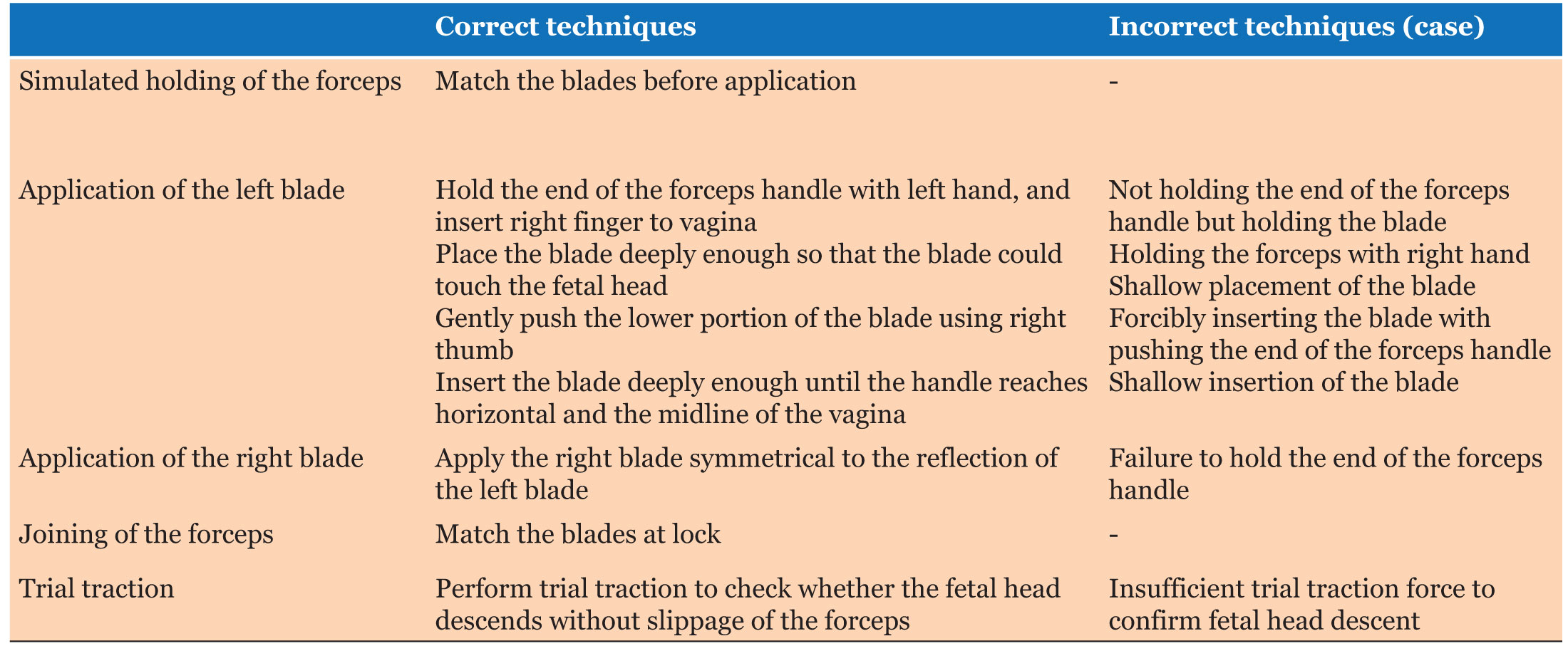
This video shows a novice obstetrician attempting her first forceps delivery under the supervision of a specialist, after completion of the simulation training program. The specialist will take over if there is any risk to the patient. The novice obstetrician was in her fourth year of training, which included 2 years of medical internship. The forceps delivery was supervised by an obstetrician with 16 years of experience. The second stage of labor was prolonged by uterine inertia despite oxytocin augmentation. As no further fetal descent was anticipated, a decision was made to deliver the baby using UTokyo Naegele forceps (ATOM Medical) from fetal head station +4. The patient agreed to video recording of the forceps delivery. The forceps delivery was accomplished without any complications; however, there was still room for improvement. In this section, we demonstrate the points to note using video captions (Video 1), (Table 1).
Insertion of the forceps with hands reversed
During the insertion of the left blade of the forceps, the right hand should be placed into the vagina for guidance and the left hand should hold the forceps. In the video, the novice was working with the hands reversed.
Holding the blade instead of the handle
For gentle application of the forceps blade, the obstetrician should hold the end of the handle without applying excessive force. In the video, the operator was holding the blade, and could not completely insert the forceps; this can also result in excessive force in the vagina, with a risk of vaginal laceration.
Overly shallow placement of the blade
The forceps has unique structural features for smooth application and delivery: the pelvic curve and the cephalic curve. Thus, appropriate application does not require intense force for suitable placement of the blade. However, to achieve appropriate placement, proper application of the forceps blade to the vulva is needed in the first step. In the video, the operator placed the forceps blade in an overly shallow position. Using the cephalic curve and placing the blade alongside the fetal head will lead to smooth application of the forceps.
Failing to insert the blade with assistance of the right thumb and forcibly inserting the blade with the left hand
During insertion, the bottom of the left forceps blade should be gently pushed into the vagina, with the right thumb on the blade. The hand holding the forceps should move vertically, but should not push the forceps. Improper technique can result in failure of forceps insertion, with a risk of vaginal laceration.
Overly shallow insertion of the blade
The operator successfully inserted the forceps; however, the blades were not placed deeply enough to join and lock both sides. The forceps should be inserted until the handle reaches the midline of the vagina and is also horizontal.
Adaptation angle is not vertical
The right blade of the forceps was attached diagonally rather than vertically.
Failure to hold the end of the handle
As for the left blade, the forceps should be held by the end of the handle.
Trial of traction force insufficient to confirm fetal head descent
A trial of traction has two goals: to confirm fetal head descent in the proper direction and to confirm the forceps will not slip off the fetal head on exiting the vagina. To verify those two points, a trial of traction should be performed at least until the fetal head begins to move.

Access video on other devices
Discussion
In this video, we demonstrate eight points where the novice obstetrician experienced setbacks. In our experience, novice obstetricians all tend to experience similar pitfalls. Thus, it is important for instructors to recognize the pitfalls of trainees. According to the video case, the novice obstetrician did not yet acquire the proper forceps delivery skill. Although the application of the forceps showed some room for improvement, the manner of traction was acceptable and the trainee was able to deliver the baby without any complications. In a case of failed forceps delivery, downward traction is usually applied incorrectly in a horizontal direction. Additionally, prolonged horizontal traction without changing to upward traction may result in severe perineal laceration. In case of a vacuum delivery, incorrect traction force direction may lead to detachment of the vacuum cup, with an injury to the fetal head. However, forceps delivery can be performed with a slightly incorrect direction of traction; this is a strength of forceps delivery, but it can also be dangerous and difficult. Thus, a novice obstetrician should learn the correct technique for forceps delivery prior to actual use.
Simulation training is effective not only for teaching a new technique but also for increasing a trainee’s confidence and self-assessment skill [5]. Recently, hands-on training, e-learning, and video learning have all been used to teach new techniques. Video learning is effective for teaching new skills [6] and maintenance of trainee motivation [7]. However, neither video alone nor simulation training is sufficient for instruction for novice obstetricians in forceps delivery. There are still some gaps between simulation training and actual clinical practice. Therein lies the significance of taking video during the clinical practice and video learning. With the relevant feedbacks of novice obstetricians’ forceps deliveries, they will realize where to improve. Accordingly, repetitive simulation training and video learning during the on-the-job training are important.
Conclusion
This is one example of forceps delivery, but we hope this video is of use to both instructors and trainees. In addition to the video learning, we think that both repetitive simulation training and on-the-job training are important.
References
1.
Takeda S, Takeda J, Koshiishi T, Makino S, Kinoshita K. Fetal station based on the trapezoidal plane and assessment of head descent during instrumental delivery. Hypertens Res Pregnancy 2014;2(2):65–71. [CrossRef]

2.
Takeda J, Makino S, Itakura A, Takeda S. Technique of forceps delivery using UTokyo Naegele forceps. Hypertens Res Pregnancy 2017;5:(1)24–5. [CrossRef]
3.
Takeda J, Makino S, Itakura A, Takeda S. Technique of rotational forceps delivery using UTokyo Kielland Forceps. Hypertens Res Pregnancy 2017;5(1):26–7.
[Pubmed]
4.
Roberts MJ, Gale TC, McGrath JS, Wilson MR. Rising to the challenge: Acute stress appraisals and selection centre performance in applicants to postgraduate specialty training in anaesthesia. Adv Health Sci Educ Theory Pract 2016 May;21(2):323–39. [CrossRef]
[Pubmed]
5.
Hilal Z, Kumpernatz AK, Rezniczek GA, Cetin C, Tempfer-Bentz EK, Tempfer CB. A randomized comparison of video demonstration versus hands-on training of medical students for vacuum delivery using objective structured assessment of technical skills (OSATS). Medicine (Baltimore) 2017 Mar;96(11):e6355. [CrossRef]
[Pubmed]
6.
De La Garza JR, Kowalewski KF, Friedrich M, et al. Does rating the operation videos with a checklist score improve the effect of E-learning for bariatric surgical training? Study protocol for a randomized controlled trial. Trials 2017 Mar 21;18(1):134. [CrossRef]
[Pubmed]
7.
Lee NJ, Chae SM, Kim H, Lee JH, Min HJ, Park DE. Mobile-based video learning outcomes in clinical nursing skill education: A randomized controlled trial. Comput Inform Nurs 2016 Jan;34(1):8–16. [CrossRef]
[Pubmed]
Supporting Information
Author Contributions:
Jun Takeda - Substantial contributions to conception and design, Acquisition of data, Analysis of data, Interpretation of data, Drafting the article, Final approval of the version to be published
Hitomi Ando - Substantial contributions to conception and design, Drafting the article, Final approval of the version to be published
Shintaro Makino - Substantial contributions to conception and design, Drafting the article, Final approval of the version to be published
Atsuo Itakura - Substantial contributions to conception and design, Revising it critically for important intellectual content, Final approval of the version to be published
Satoru Takeda - Substantial contributions to conception and design, Revising it critically for important intellectual content, Final approval of the version to be published
Competing Interests:Written informed consent was obtained from the patient for publication of this study.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}